Fill a Valid Medication Administration Record Sheet Template
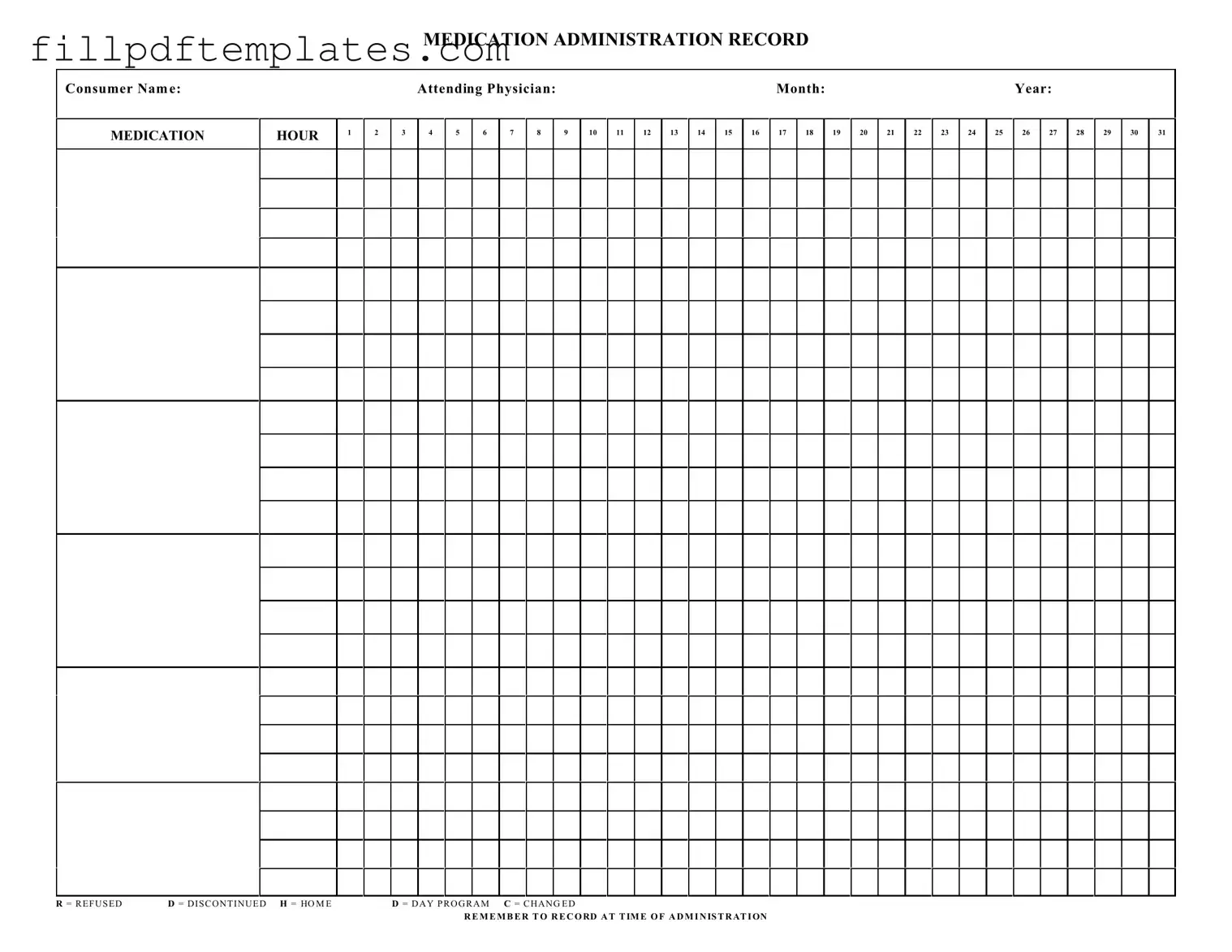
The Medication Administration Record Sheet is an essential tool used in healthcare settings to ensure that patients receive their prescribed medications accurately and on time. This form serves as a comprehensive log, capturing critical details such as the consumer's name, the attending physician, and the specific month and year of medication administration. Each day of the month is meticulously laid out, allowing healthcare providers to track medication administration hour by hour. In addition to recording the time of administration, the form includes important notations, such as R for refused, D for discontinued, H for home, D for day program, and C for changed. These notations help to provide clarity on any deviations from the prescribed regimen, ensuring that all changes are documented appropriately. By emphasizing the importance of recording medication administration at the precise time it occurs, this form not only aids in maintaining compliance with medical protocols but also enhances patient safety and care continuity.
Additional PDF Templates
Baseball Tryout Form - Collect feedback and comments for each player evaluated.
For those looking to navigate the complexities of legal decision-making, the General Power of Attorney is a vital tool that empowers an agent to act on your behalf. To ensure you have the correct resources, you can find a reliable template at arizonaformpdf.com, which will guide you through the necessary steps to complete this important document effectively.
Proposal for Building Construction - Essential for obtaining bids from contractors for construction work.
Free Bol - This form minimizes the likelihood of errors in delivery by providing clear instructions.
Similar forms
The Medication Administration Record Sheet form is similar to several other documents used in healthcare settings. Each of these documents serves a specific purpose related to medication management and patient care. Below are ten documents that share similarities with the Medication Administration Record Sheet:
- Patient Medication List: This document details all medications a patient is currently taking, including dosages and schedules, similar to how the Medication Administration Record tracks administered medications.
- Medication Reconciliation Form: This form is used to ensure that a patient's medication lists are accurate and complete, much like the Medication Administration Record helps verify what has been given to the patient.
- Hold Harmless Agreement: This document protects parties from liability during various transactions and activities, similar to a Hold Harmless Agreement that shifts risk from one party to another.
- Nursing Notes: These notes document patient care and medication administration, paralleling the Medication Administration Record's role in tracking when and what medications were given.
- Prescription Order Form: This form contains specific instructions from a physician regarding a patient's medications, which aligns with the Medication Administration Record that reflects those prescriptions being administered.
- Medication Error Report: This document is used to report any errors in medication administration, similar to how the Medication Administration Record tracks any refusals or changes in medication.
- Patient Care Plan: This outlines the overall treatment strategy for a patient, including medication management, akin to the Medication Administration Record's focus on medication administration.
- Controlled Substance Log: This log tracks the use of controlled substances, similar to how the Medication Administration Record monitors the administration of all medications.
- Medication Administration Policy: This document outlines the procedures for administering medications in a healthcare setting, which informs the practices reflected in the Medication Administration Record.
- Incident Report: This report documents any adverse events related to medication administration, much like how the Medication Administration Record can indicate issues with medication delivery.
- Daily Treatment Sheet: This sheet records all treatments and medications given to a patient throughout the day, similar to the Medication Administration Record's daily tracking of medication administration.
Document Specifics
| Fact Name | Description |
|---|---|
| Purpose | The Medication Administration Record Sheet is designed to document the administration of medications to consumers in a healthcare setting. |
| Consumer Identification | Each record must include the name of the consumer receiving the medication, ensuring accurate tracking and accountability. |
| Attending Physician | The form requires the name of the attending physician, which is essential for maintaining a clear line of communication regarding the consumer's treatment plan. |
| Monthly Tracking | Medication administration is tracked on a monthly basis, with designated spaces for each day of the month. |
| Administration Hours | The form provides a structure to record medication administration at specific hours throughout the day, ensuring timely and accurate dosing. |
| Refusal and Changes | Abbreviations such as R (Refused), D (Discontinued), and C (Changed) are included to indicate any deviations from the prescribed medication regimen. |
| Legal Compliance | In many states, the use of a Medication Administration Record is governed by healthcare regulations, such as the Nurse Practice Act, which mandates accurate documentation of medication administration. |
Things You Should Know About This Form
-
What is a Medication Administration Record Sheet?
The Medication Administration Record Sheet (MARS) is a vital tool used in healthcare settings to document the administration of medications to patients. It helps ensure that each consumer receives their prescribed medications at the correct times and in the correct dosages.
-
Who should use the Medication Administration Record Sheet?
This form is primarily used by healthcare providers, including nurses and caregivers, who are responsible for administering medications to patients. It is also useful for family members who may be managing medications for loved ones at home.
-
What information is required on the form?
The MARS requires essential details such as the consumer's name, the attending physician's name, the month and year, and a grid for recording medication administration times. It also includes codes for documenting if medications were refused, discontinued, or changed.
-
How do I record medication administration?
To record medication administration, simply fill in the appropriate box corresponding to the hour when the medication was given. You can mark an "R" if the medication was refused, "D" if it was discontinued, or "C" if there was a change in the medication. Always remember to record at the time of administration for accuracy.
-
Why is it important to keep accurate records?
Accurate records are crucial for ensuring patient safety. They help prevent medication errors, allow healthcare providers to track the effectiveness of treatments, and provide valuable information for future medical decisions. Inaccurate records can lead to serious health risks.
-
How long should I keep the Medication Administration Record Sheet?
It is recommended to keep the MARS for a specified period, typically ranging from three to seven years, depending on state regulations and healthcare facility policies. This retention period allows for proper review and auditing of medication administration practices.
-
Can I use the form for multiple consumers?
No, the Medication Administration Record Sheet is designed for individual consumers. Each consumer should have their own record sheet to ensure accurate tracking of their medications and to maintain confidentiality.
-
What should I do if I make a mistake on the form?
If you make a mistake while filling out the MARS, it is important to correct it properly. Cross out the error with a single line, and initial and date the correction. This practice maintains the integrity of the record while ensuring that the correct information is clear.
Documents used along the form
The Medication Administration Record Sheet is a crucial document in the healthcare setting, ensuring that patients receive their medications accurately and on time. Alongside this form, several other documents help maintain comprehensive records and enhance the quality of care provided to consumers. Below is a list of related forms and documents that are often utilized in conjunction with the Medication Administration Record Sheet.
- Patient Information Sheet: This document contains essential details about the patient, including their medical history, allergies, and current medications. It serves as a foundational reference for healthcare providers.
- Medication Order Form: This form outlines the specific medications prescribed by a physician. It includes dosage, frequency, and route of administration, ensuring clarity in the treatment plan.
- Informed Consent Form: Before administering certain medications or treatments, healthcare providers often require patients to sign this document. It confirms that the patient understands the risks and benefits associated with the proposed treatment.
- Incident Report Form: In the event of an adverse reaction or medication error, this form documents the incident. It is vital for quality assurance and helps prevent future occurrences.
- Transfer-on-Death Deed Form: Property owners can secure their legacy with a clear designation of beneficiaries, allowing a seamless transfer of real estate upon their death, avoiding probate complications. For more details, you can visit todform.com/blank-arizona-transfer-on-death-deed.
- Medication Reconciliation Form: This document is used to compare a patient's current medications with their prescribed medications during transitions of care. It helps identify discrepancies and ensures continuity of care.
- Care Plan: This comprehensive document outlines the overall treatment strategy for the patient, including goals, interventions, and expected outcomes. It integrates medication management with other aspects of care.
- Progress Notes: These notes provide ongoing documentation of the patient's condition and response to treatment. They are essential for tracking changes over time and informing future care decisions.
Utilizing these documents in conjunction with the Medication Administration Record Sheet enhances the overall effectiveness of patient care. By maintaining thorough and accurate records, healthcare providers can ensure that each patient receives the best possible treatment tailored to their individual needs.
Medication Administration Record Sheet Preview
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON