Fill a Valid Cna Shower Sheets Template
The CNA Shower Sheets form is an essential tool in the realm of resident care, particularly during bathing routines. This form serves multiple purposes, primarily focusing on the visual assessment of a resident's skin condition while they receive a shower. Care aides are tasked with observing any abnormalities, such as bruising, skin tears, rashes, or lesions, and must report these findings to the charge nurse immediately. The form includes a body chart that allows caregivers to accurately document the location and description of any skin issues noted during the assessment. Furthermore, it prompts the caregiver to check for additional concerns, such as the need for toenail care. After the initial assessment, the charge nurse reviews the findings, providing their signature and any necessary interventions. If further action is required, the information can be forwarded to the Director of Nursing (DON) for additional oversight. This systematic approach not only enhances the quality of care provided but also ensures that any skin-related issues are addressed promptly, contributing to the overall well-being of residents.
Additional PDF Templates
Sample Incident Report - Encourages reporting of near-miss incidents to improve safety.
For more information on how to obtain a Sample Tax Return Transcript, you can visit legalpdfdocs.com, where you will find helpful resources and templates to assist you in the process.
How to Put a Lien on a House in Florida - Property owners should read this notice carefully to understand the implications of non-payment.
Profit and Loss Statement Template - Maintenance of this form can enhance decision-making processes.
Similar forms
Skin Assessment Form: Similar to the CNA Shower Sheets, this document focuses on the evaluation of skin integrity. It requires caregivers to document any abnormalities, ensuring timely reporting and intervention.
Incident Report: This form captures any unusual occurrences during care, including skin issues. Like the CNA Shower Sheets, it emphasizes the importance of documentation and communication with nursing staff.
Patient Care Plan: This document outlines the strategies for managing a resident’s health needs. It parallels the CNA Shower Sheets by including assessments of skin conditions as part of the overall care strategy.
- Articles of Incorporation: Essential for establishing a corporation in Washington State, the Articles of Incorporation form legally documents the creation of the company, including details such as the corporation's name, purpose, and initial directors.
Daily Care Log: This log records daily interactions and observations. It is similar to the CNA Shower Sheets in that it requires detailed documentation of any skin abnormalities noted during routine care.
Wound Care Assessment: This form specifically addresses wounds and their healing progress. It shares a similar purpose with the CNA Shower Sheets, focusing on identifying and documenting skin issues.
Medication Administration Record (MAR): While primarily for medications, it often includes notes on skin reactions to drugs. This document aligns with the CNA Shower Sheets by promoting awareness of skin health in relation to treatments.
Fall Risk Assessment: This assessment evaluates a resident's risk of falling, which can be related to skin integrity. It shares a common goal with the CNA Shower Sheets of preventing further health complications.
Vital Signs Record: This document tracks essential health metrics. It is similar in that it often includes skin temperature and color as indicators of overall health status.
Transfer Summary: When a resident is moved to a different care setting, this summary includes health assessments, including skin conditions. It reflects the same need for thorough documentation as the CNA Shower Sheets.
Document Specifics
| Fact Name | Details |
|---|---|
| Purpose | The CNA Shower Sheets form is used for documenting skin assessments during resident showers. |
| Skin Monitoring | It requires a comprehensive visual assessment of a resident’s skin for abnormalities. |
| Reporting | Any abnormal findings must be reported to the charge nurse immediately. |
| Documentation | The form includes a body chart for graphing the exact location of skin abnormalities. |
| Assessment Items | The form lists 15 specific skin conditions to assess, including bruising and rashes. |
| Toenail Care | The form inquires whether the resident needs toenail trimming, with a Yes/No option. |
| Signatures Required | Signatures from both the CNA and the charge nurse are required for validation. |
| Forwarding Issues | Any problems identified must be forwarded to the Director of Nursing (DON) for review. |
| Governing Law | This form is governed by regulations under the Centers for Medicare & Medicaid Services (CMS). |
Things You Should Know About This Form
-
What is the purpose of the CNA Shower Sheets form?
The CNA Shower Sheets form is designed for certified nursing assistants (CNAs) to document a resident's skin condition during showers. It helps in identifying and reporting any abnormalities in the skin, ensuring that appropriate care is provided.
-
Who should use the CNA Shower Sheets form?
This form should be used by CNAs when they are responsible for bathing residents. It is a vital tool for monitoring skin health and ensuring that any issues are promptly reported to the charge nurse.
-
What types of skin conditions should be assessed?
CNAs should assess for various skin conditions, including:
- Bruising
- Skin tears
- Rashes
- Swelling
- Dryness
- Soft heels
- Lesions
- Decubitus (pressure sores)
- Blisters
- Scratches
- Abnormal color
- Abnormal skin texture or temperature
- Other abnormalities
-
How should abnormalities be documented?
Abnormalities should be documented using the provided body chart on the form. CNAs must describe and graph the location and nature of each abnormality by number, ensuring clarity in reporting.
-
What should be done if an abnormality is found?
If a CNA identifies any abnormal skin condition, they must report it to the charge nurse immediately. The charge nurse will then assess the situation and determine the necessary interventions.
-
Is there a section for toenail care?
Yes, the form includes a section to indicate whether the resident needs their toenails cut. CNAs should assess this during the shower and mark their findings accordingly.
-
What happens after the charge nurse assesses the resident?
After the charge nurse conducts their assessment, they will document their findings and any recommended interventions on the form. This information may be forwarded to the Director of Nursing (DON) for further review if necessary.
-
How is the form submitted or stored?
The completed form should be submitted to the appropriate nursing staff for record-keeping. It is essential to ensure that all documentation is accurate and stored securely to maintain resident confidentiality.
-
Where can I find more information about the CNA Shower Sheets form?
Additional information about the CNA Shower Sheets form can be found at www.primaris.org. This site provides resources related to quality improvement in healthcare.
-
Is this form a requirement for all residents?
While it is recommended for all residents, the use of the CNA Shower Sheets form may vary based on facility policies and individual resident needs. It is important to follow your facility's guidelines.
Documents used along the form
When working with the CNA Shower Sheets form, several other documents may be needed to ensure comprehensive care and documentation for residents. Each of these forms plays a vital role in maintaining quality standards and facilitating communication among staff members. Here’s a list of documents that are often used alongside the CNA Shower Sheets:
- Resident Assessment Protocol (RAP): This document provides a detailed evaluation of a resident's overall health, including physical, mental, and emotional aspects. It helps in creating a personalized care plan.
- Care Plan: A care plan outlines the specific needs and goals for a resident based on assessments. It includes strategies for addressing health issues and improving quality of life.
- Skin Integrity Assessment Form: This form is used to document the condition of a resident's skin over time, tracking changes and noting any interventions taken to prevent skin breakdown.
- Incident Report: If any unusual events occur during care, such as a fall or injury, this report is completed to document the incident, the response, and any follow-up actions taken.
- Daily Care Log: Staff members use this log to record daily activities and observations related to a resident's care, including hygiene, mobility, and interactions.
- Last Will and Testament: It is essential to have a plan in place, which is why you should consider our comprehensive Last Will and Testament guidelines to protect your wishes after passing.
- Medication Administration Record (MAR): This document tracks all medications given to a resident, including dosages and times, ensuring proper medication management.
- Vital Signs Record: This form is used to document a resident’s vital signs, such as temperature, pulse, and blood pressure, providing essential information for ongoing health assessments.
- Nutrition and Hydration Record: This document tracks a resident's food and fluid intake, ensuring that their nutritional needs are being met and identifying any issues related to hydration.
- Behavioral Health Assessment: This form assesses a resident's mental and emotional well-being, identifying any concerns that may require intervention or support.
These documents work together to create a comprehensive picture of a resident's health and well-being. Properly maintaining and utilizing these forms ensures that all staff members are informed and equipped to provide the best care possible.
Cna Shower Sheets Preview
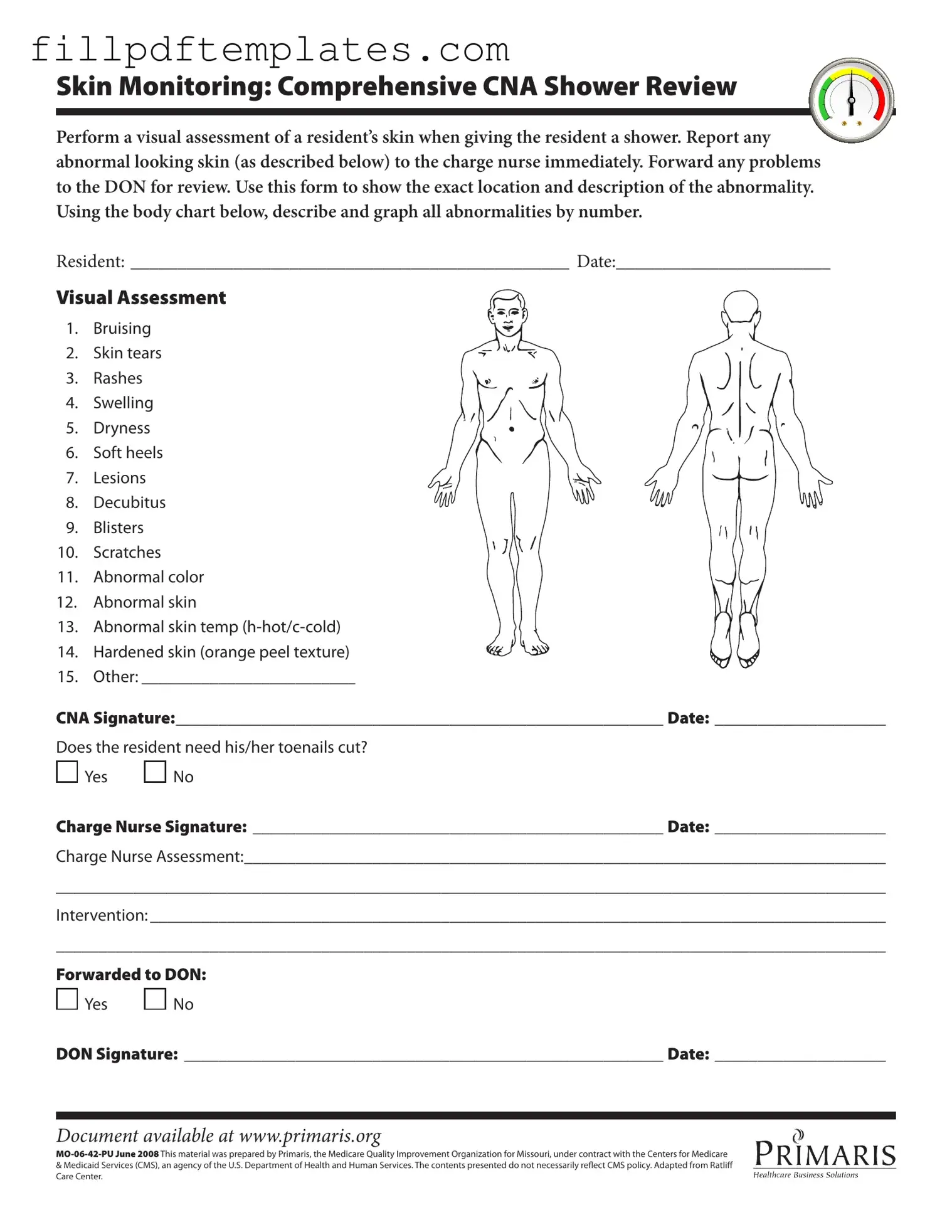
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.