Fill a Valid Annual Physical Examination Template
The Annual Physical Examination form serves as a comprehensive tool designed to gather essential health information from patients prior to their medical appointments. This form is divided into two main parts, each focusing on different aspects of the patient’s health. In the first part, patients are required to provide personal details such as their name, date of birth, and address, along with information about any significant health conditions or diagnoses they may have. It also includes a section for current medications, detailing the names, dosages, and prescribing physicians, ensuring that healthcare providers have a clear understanding of the patient's medication regimen. Additionally, the form asks about allergies, immunizations, and recent medical tests, such as tuberculosis screenings and various diagnostic procedures. The second part of the form focuses on the general physical examination, where vital signs like blood pressure and pulse are recorded. It also includes an evaluation of different body systems, allowing healthcare providers to assess the patient's overall health status. This thorough approach not only facilitates effective communication between patients and healthcare providers but also helps in identifying any potential health issues that may need further attention.
Additional PDF Templates
Panel Load Calculation - Completion of this form is a step toward responsible energy consumption.
Free Printable Direction to Pay Form - Expressly state your consent for the insurance company to issue payment directly to the repair shop.
Utilizing the New Jersey Transfer-on-Death Deed can significantly streamline the process of passing down your property, ensuring that it reaches your chosen beneficiaries smoothly and efficiently. For detailed guidance on how to properly complete this essential legal document, you can visit transferondeathdeedform.com/new-jersey-transfer-on-death-deed, which offers valuable resources to facilitate your estate planning.
Form 4506t - Identifiable data points make this document useful for verification in financial transactions.
Similar forms
-
Medical History Form: This document gathers a patient's comprehensive medical history, including past illnesses, surgeries, and family health background. Similar to the Annual Physical Examination form, it aims to provide healthcare professionals with essential information to inform treatment and care decisions.
-
Immunization Record: This record tracks a patient’s vaccination history, including dates and types of vaccines received. Like the Annual Physical Examination form, it ensures that healthcare providers have up-to-date information on a patient’s immunization status, which is crucial for preventive care.
-
Medication List: This document outlines all medications a patient is currently taking, including dosages and prescribing physicians. It serves a similar purpose to the medication section of the Annual Physical Examination form, facilitating medication management and reducing the risk of drug interactions.
-
Lab Test Results Form: This form details the outcomes of various lab tests performed on a patient, such as blood work or urinalysis. It parallels the diagnostic tests section of the Annual Physical Examination form, providing critical insights into a patient's health status.
-
Referral Form: This document is used when a healthcare provider recommends a patient see a specialist. It shares similarities with the specialty consults section of the Annual Physical Examination form, ensuring continuity of care and appropriate follow-up.
- Hold Harmless Agreement: Essential in various business and personal scenarios, the Hold Harmless Agreement serves to protect one party from liability for any injuries or damages suffered by another party, especially crucial under specific Alabama state laws.
-
Discharge Summary: Upon leaving a hospital or clinic, patients receive this summary, which includes treatment received and follow-up instructions. Like the Annual Physical Examination form, it aims to ensure that patients understand their ongoing health needs and care plans.
-
Patient Consent Form: This document secures a patient's consent for treatment or procedures. It is akin to the consent obtained during the Annual Physical Examination process, emphasizing the importance of patient autonomy and informed decision-making.
-
Health Risk Assessment: This assessment evaluates a patient's risk factors for various health conditions. Similar to the evaluation of systems in the Annual Physical Examination form, it helps identify areas needing attention for preventive care.
-
Follow-Up Care Plan: This plan outlines the next steps in a patient’s treatment after an examination or procedure. It mirrors the recommendations section of the Annual Physical Examination form, guiding patients on what to do next for optimal health.
-
Wellness Screening Questionnaire: This questionnaire assesses lifestyle factors affecting a patient's health, such as diet and exercise. It is similar to the recommendations for health maintenance in the Annual Physical Examination form, focusing on preventive measures and overall wellness.
Document Specifics
| Fact Name | Details |
|---|---|
| Purpose of the Form | The Annual Physical Examination form collects essential health information to ensure comprehensive medical evaluations and continuity of care. |
| Required Information | Patients must provide personal details, medical history, current medications, allergies, and immunization records to avoid delays in their appointments. |
| Screening Recommendations | Regular screenings for conditions such as tuberculosis, prostate health, and mammograms are advised based on age and gender, ensuring proactive health management. |
| State-Specific Laws | In California, the governing law for physical examinations is outlined in the California Business and Professions Code, Section 2052, which mandates the need for annual health assessments. |
Things You Should Know About This Form
-
What is the purpose of the Annual Physical Examination form?
The Annual Physical Examination form is designed to gather essential health information before your medical appointment. This information helps healthcare providers assess your overall health, identify any potential issues, and create a personalized care plan. Completing this form accurately can prevent delays and ensure a thorough examination.
-
What information is required in Part One of the form?
Part One of the form requires personal details such as your name, date of birth, address, and Social Security Number. Additionally, you will need to provide information about any significant health conditions, current medications, allergies, and immunizations. This section is crucial for your healthcare provider to understand your medical history and current health status.
-
How do I report my current medications?
In the medications section, list each medication you are currently taking, including the name, dosage, frequency, and the diagnosis for which it was prescribed. If you need more space, feel free to attach an additional page. Indicate whether you take these medications independently, as this information is vital for your healthcare provider.
-
What are the immunization requirements listed on the form?
The form asks for information on several immunizations, including Tetanus/Diphtheria, Hepatitis B, Influenza, and Pneumovax. You should provide the dates of administration and the type of vaccine received. Keeping this information updated is essential for your health and can help prevent diseases.
-
What should I include in the section about allergies?
In the allergies section, list any known allergies or sensitivities you have. This includes reactions to medications, foods, or environmental factors. Providing this information allows your healthcare provider to avoid prescribing medications or treatments that could cause adverse reactions.
-
What is the significance of the tuberculosis (TB) screening?
The TB screening section is important for identifying potential exposure to tuberculosis. If you have had a TB test, you will need to provide the date it was administered, the date it was read, and the results. If the test is positive, additional steps such as a chest x-ray may be necessary to ensure your health and the safety of others.
-
How often should I have my physical examination?
It is generally recommended that adults have an annual physical examination. However, the frequency may vary based on individual health needs, age, and risk factors. Your healthcare provider can give you specific recommendations based on your personal health history.
-
What happens if I don't complete the form before my appointment?
If you do not complete the form prior to your appointment, it may result in delays. Your healthcare provider may need to gather this information during your visit, which could prolong your wait time and limit the time available for your examination.
-
Can I update my information if my health status changes?
Yes, it is important to update your information if your health status changes. If you experience new health conditions, changes in medication, or any other significant health updates, inform your healthcare provider during your appointment. Keeping your records current ensures you receive the best possible care.
Documents used along the form
The Annual Physical Examination form is an essential document for assessing a person's health. However, several other forms and documents often accompany it to provide a comprehensive view of an individual's medical history and needs. Below is a list of these additional forms, each serving a specific purpose.
- Medical History Form: This document collects detailed information about a patient's past illnesses, surgeries, and family medical history. It helps healthcare providers understand risk factors and tailor care accordingly.
- Medication List: A comprehensive list of all medications a patient is currently taking, including dosages and frequencies. This ensures that healthcare providers are aware of potential drug interactions and can make informed decisions.
- Immunization Record: This form tracks all vaccinations a patient has received. It is crucial for assessing immunity and determining if any additional vaccines are needed.
- Lab Test Results: Results from any recent laboratory tests, such as blood work or urinalysis, are included to provide insights into the patient's current health status and any underlying conditions.
- Referral Form: If a specialist's consultation is necessary, a referral form may be used. This document outlines the reason for the referral and any relevant medical history.
- Motorcycle Bill of Sale: This legal document records the transfer of motorcycle ownership, protecting both buyer and seller. For details, refer to the legalpdfdocs.com/.
- Patient Consent Form: This form ensures that the patient understands and agrees to the procedures and treatments recommended by the healthcare provider. It protects both the patient and the provider legally.
- Advance Directive: A legal document that outlines a patient's wishes regarding medical treatment in case they become unable to communicate their preferences. This is important for ensuring that a patient’s desires are respected.
- Insurance Information Form: This form captures details about the patient’s health insurance coverage. It is necessary for billing purposes and to verify coverage for services rendered.
- Follow-Up Care Plan: After the examination, a follow-up care plan may be provided. This document outlines any recommended next steps, including further tests, referrals, or lifestyle changes.
These documents, when used alongside the Annual Physical Examination form, create a thorough picture of a patient's health. They ensure that healthcare providers can deliver informed and effective care tailored to individual needs.
Annual Physical Examination Preview
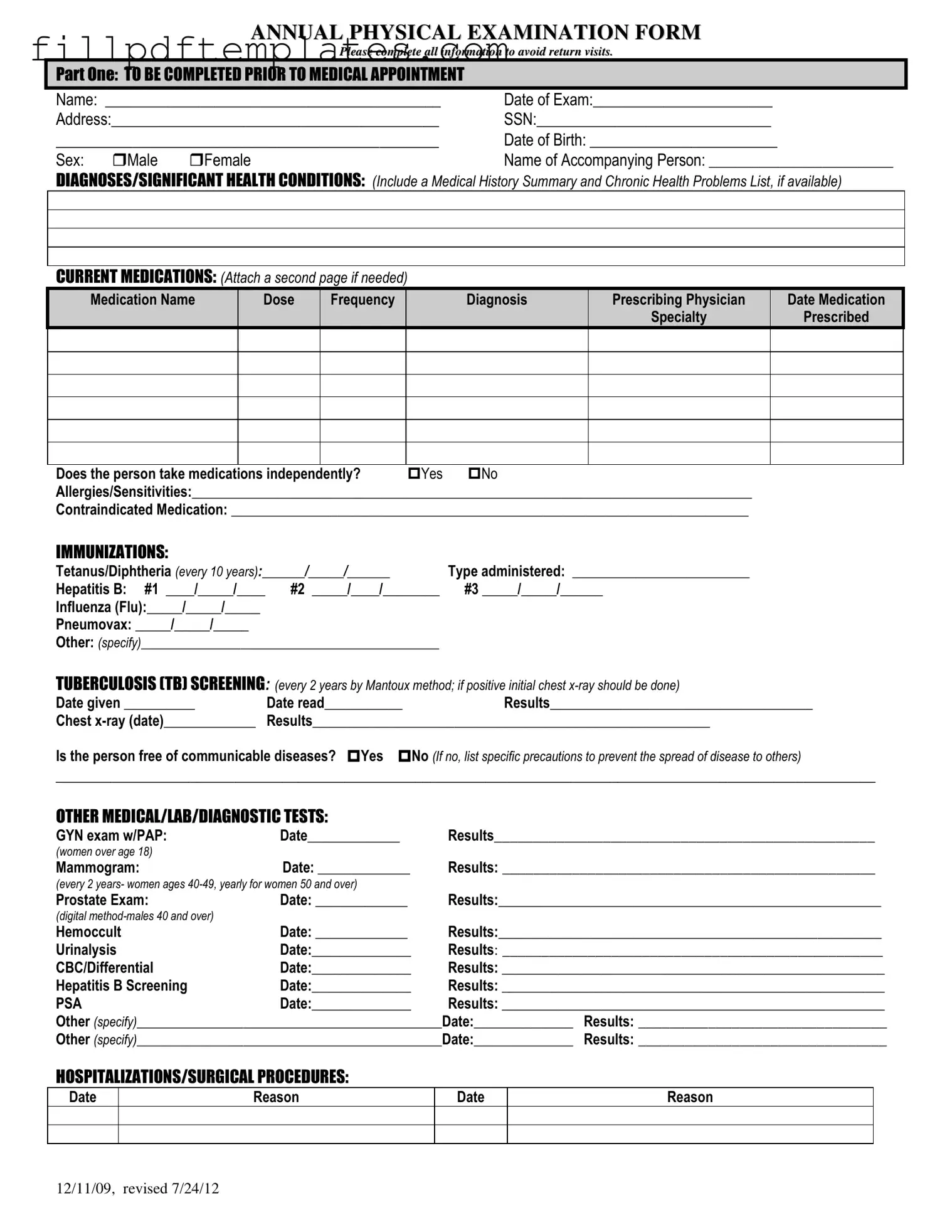
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12

PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12