Fill a Valid Advance Beneficiary Notice of Non-coverage Template
The Advance Beneficiary Notice of Non-coverage, often referred to as the ABN, plays a crucial role in the healthcare landscape, particularly for Medicare beneficiaries. This form serves as a communication tool between healthcare providers and patients, informing individuals when a service may not be covered by Medicare. By receiving an ABN, patients gain insight into their potential financial responsibilities before undergoing specific procedures or treatments. The form outlines the reasons for non-coverage, allowing patients to make informed decisions about their care. It also provides an opportunity for beneficiaries to understand their rights and options, including the ability to accept or refuse the service in question. Understanding the ABN is essential for navigating the complexities of Medicare coverage and ensuring that patients are not caught off guard by unexpected costs. This article will delve into the intricacies of the ABN, exploring its purpose, the circumstances under which it is issued, and the implications for both patients and healthcare providers.
Additional PDF Templates
Section 8 100 Gold Street - Be proactive to avoid any potential complications with your housing assistance.
To facilitate a smooth rental process, you can utilize a standard Lease Agreement form template that outlines key terms and responsibilities between landlords and tenants, ensuring clarity in your leasing arrangements.
Four Point Inspection Florida - Inspectors must indicate the actual year the property was built to provide context for the inspection results.
Similar forms
- Informed Consent Form: Like the Advance Beneficiary Notice of Non-coverage, this document ensures that patients understand the risks and benefits of a procedure before agreeing to it. Both forms serve to protect patient rights and provide transparency in healthcare decisions.
- Patient Authorization Form: This document allows healthcare providers to obtain permission from patients to share their medical information. Similar to the Advance Beneficiary Notice, it emphasizes the importance of patient consent and awareness regarding their healthcare.
- Notice of Privacy Practices: This document informs patients about how their medical information may be used and disclosed. Both forms aim to educate patients about their rights and the handling of their personal health information.
- Financial Responsibility Agreement: Patients sign this document to acknowledge their responsibility for payment of services rendered. Like the Advance Beneficiary Notice, it clarifies financial obligations and helps prevent misunderstandings.
- Medicare Summary Notice: This notice provides beneficiaries with details about the services they received and the costs involved. Both documents help patients understand their coverage and any potential out-of-pocket expenses.
- Advance Directive: This legal document outlines a patient’s wishes regarding medical treatment in case they become unable to communicate. Similar to the Advance Beneficiary Notice, it promotes patient autonomy and informed decision-making.
- Patient Discharge Instructions: These instructions inform patients about their care after leaving a healthcare facility. Like the Advance Beneficiary Notice, they ensure that patients are aware of their ongoing health needs and responsibilities.
- Hold Harmless Agreement: This legal document transfers risk from one party to another, ensuring that one party will not hold the other responsible for any loss or damage, similar to how certain documents inform beneficiaries about potential risks. For more information, you can visit the Hold Harmless Agreement.
- Referral Authorization Form: This form is used when a primary care physician refers a patient to a specialist. Both documents emphasize the importance of communication and consent in the healthcare process.
- Insurance Verification Form: This document confirms a patient’s insurance coverage before services are rendered. Similar to the Advance Beneficiary Notice, it aims to clarify coverage details and avoid unexpected costs.
- Treatment Plan Agreement: This outlines the proposed treatment and the patient’s agreement to it. Like the Advance Beneficiary Notice, it fosters understanding and agreement between the patient and provider regarding care.
Document Specifics
| Fact Name | Details |
|---|---|
| Purpose | The Advance Beneficiary Notice of Non-coverage (ABN) informs Medicare beneficiaries that a service may not be covered. |
| Who Issues It | Healthcare providers issue the ABN to patients before providing services that may not be reimbursed by Medicare. |
| When to Use | Providers should use the ABN when they believe Medicare will deny payment for a service or item. |
| Beneficiary Rights | Patients have the right to refuse the service if they do not want to pay out of pocket. |
| State-Specific Forms | Some states may have specific versions of the ABN, governed by local Medicare laws. |
| Signature Requirement | Beneficiaries must sign the ABN to acknowledge they understand the potential non-coverage. |
| Implications of Non-Signing | If a beneficiary does not sign, they may still be responsible for payment if Medicare denies coverage. |
Things You Should Know About This Form
-
What is the Advance Beneficiary Notice of Non-coverage (ABN)?
The Advance Beneficiary Notice of Non-coverage, commonly referred to as the ABN, is a form that healthcare providers use to inform Medicare beneficiaries that a service or item may not be covered by Medicare. This notice is important because it helps beneficiaries understand their potential financial responsibilities before receiving services.
-
When should I receive an ABN?
You should receive an ABN before a service is provided if your healthcare provider believes that Medicare may not cover the service. This could happen for various reasons, such as the service being deemed not medically necessary or not meeting Medicare’s coverage criteria. Receiving this notice allows you to make informed decisions about your care and any potential costs.
-
What happens if I don’t sign the ABN?
If you choose not to sign the ABN, your healthcare provider may still provide the service, but you may be responsible for the full cost if Medicare denies coverage. By signing the ABN, you acknowledge that you understand the potential financial implications and agree to take responsibility for payment if Medicare does not cover the service.
-
Can I appeal if Medicare denies coverage after I sign the ABN?
Yes, you can appeal Medicare's decision if you believe the service should be covered. Signing the ABN does not waive your right to appeal. You will need to follow Medicare’s appeal process, which typically involves submitting a request for reconsideration and providing any necessary documentation to support your case.
-
What should I do if I have questions about the ABN?
If you have questions about the ABN or its implications, it is best to speak directly with your healthcare provider. They can explain the specific reasons for the notice and help you understand your options. Additionally, you can contact Medicare directly for more information about coverage and your rights as a beneficiary.
Documents used along the form
The Advance Beneficiary Notice of Non-coverage (ABN) form is an important document in healthcare that informs patients when a service may not be covered by Medicare. Alongside the ABN, there are several other forms and documents that healthcare providers often use to ensure clarity and compliance. Below is a list of commonly associated forms.
- Medicare Summary Notice (MSN): This document summarizes the services provided to a Medicare beneficiary, detailing what was billed, what Medicare paid, and any remaining patient responsibilities.
- Notice of Exclusions from Medicare Benefits (NEMB): This notice informs beneficiaries about services that are excluded from Medicare coverage, helping them understand their financial obligations.
- Patient Consent Form: This form secures a patient's consent for treatment or services, ensuring that they are informed about what to expect and any potential costs involved.
- Transfer-on-Death Deed: This legal document allows for the direct transfer of real estate to beneficiaries upon death without the probate process, providing peace of mind for property owners. For more details, visit https://todform.com/blank-massachusetts-transfer-on-death-deed.
- Claim Form (CMS-1500): This form is used by healthcare providers to bill Medicare for services rendered. It captures essential details about the patient, provider, and services provided.
- Financial Responsibility Agreement: This document outlines the patient's financial obligations for services not covered by insurance, clarifying payment expectations before treatment begins.
Understanding these documents helps patients navigate their healthcare options and financial responsibilities. Each form plays a crucial role in maintaining transparency and ensuring informed decision-making in the healthcare process.
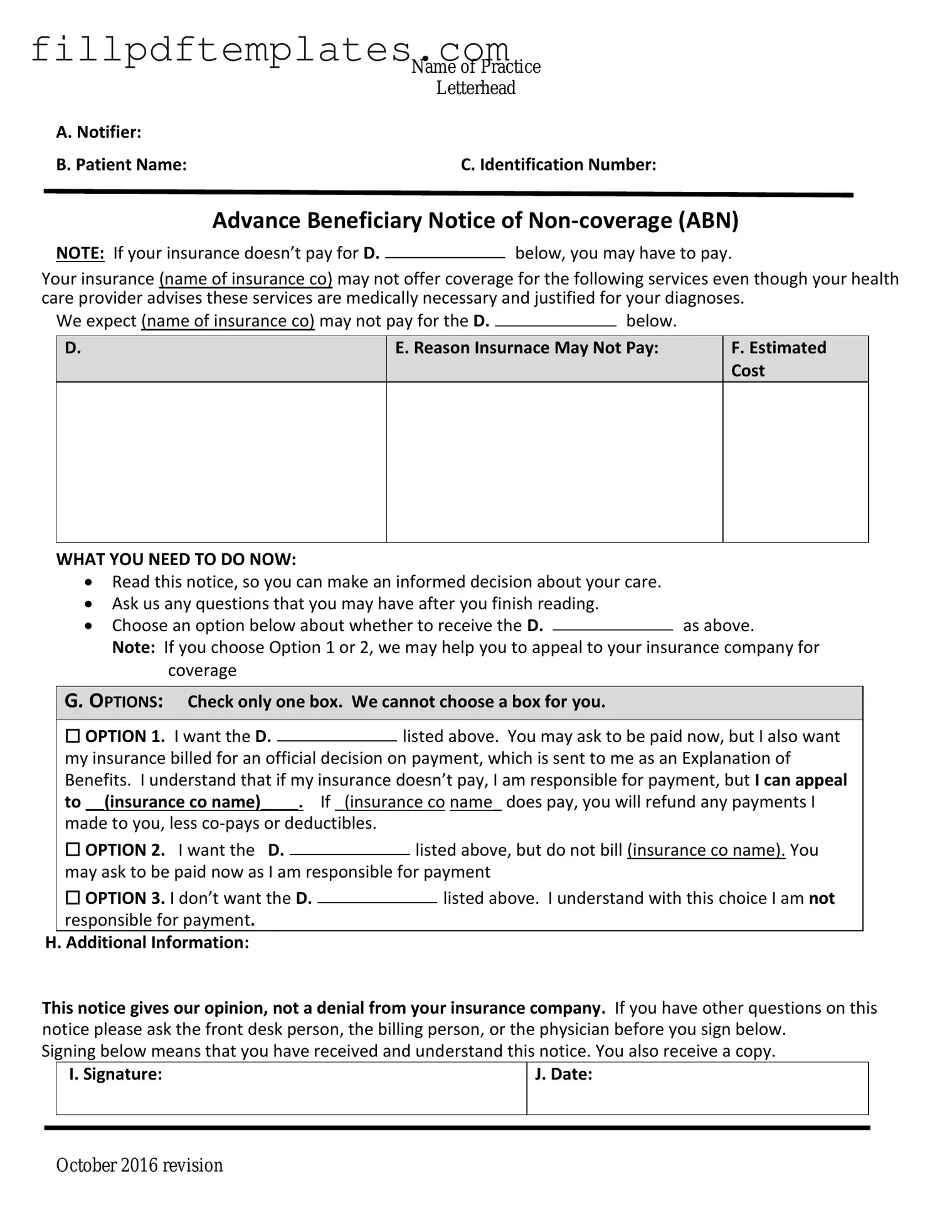
Advance Beneficiary Notice of Non-coverage Preview
|
Name of Practice |
|
Letterhead |
A. Notifier: |
|
B. Patient Name: |
C. Identification Number: |
Advance Beneficiary Notice of
NOTE: If your insurance doesn’t pay for D.below, you may have to pay.
Your insurance (name of insurance co) may not offer coverage for the following services even though your health care provider advises these services are medically necessary and justified for your diagnoses.
We expect (name of insurance co) may not pay for the D. |
|
below. |
|
D.
E. Reason Insurnace May Not Pay:
F.Estimated Cost
WHAT YOU NEED TO DO NOW:
Read this notice, so you can make an informed decision about your care.
Ask us any questions that you may have after you finish reading.
Choose an option below about whether to receive the D.as above.
Note: If you choose Option 1 or 2, we may help you to appeal to your insurance company for coverage
G. OPTIONS: Check only one box. We cannot choose a box for you.
|
☐ OPTION 1. I want the D. |
|
listed above. You may ask to be paid now, but I also want |
||||
|
|
||||||
|
my insurance billed for an official decision on payment, which is sent to me as an Explanation of |
||||||
|
Benefits. I understand that if my insurance doesn’t pay, I am responsible for payment, but I can appeal |
||||||
|
to __(insurance co name)____. If _(insurance co name_ does pay, you will refund any payments I |
||||||
|
made to you, less |
|
|
|
|||
|
☐ OPTION 2. I want the D. |
|
|
listed above, but do not bill (insurance co name). You |
|||
|
|
|
|||||
|
may ask to be paid now as I am responsible for payment |
||||||
|
☐ OPTION 3. I don’t want the D. |
|
|
|
listed above. I understand with this choice I am not |
||
|
|
|
|
||||
|
responsible for payment. |
|
|
|
|||
H. Additional Information: |
|
|
|
||||
This notice gives our opinion, not a denial from your insurance company. If you have other questions on this notice please ask the front desk person, the billing person, or the physician before you sign below.
Signing below means that you have received and understand this notice. You also receive a copy.
|
I. Signature: |
J. Date: |
|
|
|
|
|
|
October 2016 revision